SHA vs. Linda Mama: Why Kenyan Mothers Are Now Paying For Care That Was Once Free
L
Leisure Collective
Author
181
0
0
Linda Mama was not perfect. But it was free. Then SHA promised something better — and then underfunded it by 70%. Now, Kenyan mothers are reaching into empty pockets at the delivery table. Here's what happened.
There is a phrase Kenyan midwives have started hearing at delivery rooms across the country:
"But I thought it was covered."
She is 28 weeks into her pregnancy. She registered on the SHA portal like she was told to. She went to her antenatal appointments. She did everything right.
And now she is being handed a bill.
This is the quiet collapse happening inside Kenya's maternal health system — and most people don't even know it started the day Linda Mama ended.
What Linda Mama Was — And What It Promised
The Linda Mama programme, run under the old National Hospital Insurance Fund (NHIF), was Kenya's flagship free maternity programme. For all its bureaucratic imperfections, its promise was simple: show up pregnant, give birth, go home without paying a delivery fee.
It was not universal. Coverage was patchy in private facilities. Rural women faced referral barriers. NHIF had its own well-documented problems with fraud and inefficiency. But for millions of Kenyan women — especially those in the informal sector — Linda Mama was a genuine financial lifeline.
In October 2024, the Social Health Authority (SHA) officially took over, replacing NHIF and introducing the Social Health Insurance Fund (SHIF). The government called it a revolution. A step toward Universal Health Coverage.
What it became, for many mothers, was a wall.
What Changed — And What Got Lost
Under the SHA's new structure, maternity care is distributed across three separate funds — the Primary Healthcare Fund (PHCF), the Social Health Insurance Fund (SHIF), and the Emergency, Chronic and Critical Illness Fund (ECCIF). Antenatal and postnatal care fall under the PHCF. Delivery services sit under SHIF.
On paper, the SHA benefit package is described as more comprehensive than Linda Mama — with higher reimbursement rates for providers and broader service categories.
In practice, it is severely underfunded.
According to a ThinkWell analysis, the government allocated only KES 7.1 billion for the PHCF in FY 2024/25 — representing just 16% of the required budget. For FY 2025/26, allocation improved to KES 13.1 billion, still only 30% of what is needed to deliver the promised services.
The SHA itself is running a deficit. According to KNBS data, SHA losses have reached KSh 91.5 billion, with monthly SHIF collections averaging KSh 6.5 billion against a required KSh 8.3 billion.
You cannot fund universal health coverage at 16% of budget and call it free.
The Provider Squeeze — And Who Pays For It
When the government underfunds the system, the pressure cascades downward — onto health facilities, and then onto patients.
A Rural Private Health Association (RUPHA) survey conducted between April and May 2025 found that only 20% of Primary Healthcare-accredited facilities received SHA payments every month during the January–March 2025 quarter. Forty-five percent received no PHC payments at all during that period.
RUPHA threatened to suspend credit services to SHA patients entirely over unpaid reimbursement claims.
Many SHA tariffs do not reflect the real cost of delivering care. They do not cover medications, consumables, diagnostics, imaging, or specialist fees in full. So what do facilities do? They charge the patient the difference.
This is why a woman who registered with SHA, attended all her antenatal visits, and delivered at an accredited facility can still walk out — or worse, be detained — with a bill she cannot pay.
The shift from Linda Mama to SHA has been linked to early signs of declining skilled birth attendance — meaning more women may be turning to home births or unqualified attendants to avoid the cost. The consequences of that choice are measured in maternal deaths.
The Numbers Behind The Crisis
Kenya's maternal mortality stands at 355 deaths per 100,000 live births — roughly 15 mothers and 92 newborns dying every single day from largely preventable causes. This was the national reality even before SHA introduced new financial barriers.
The leading causes of maternal death in Kenya are postpartum haemorrhage (40%), obstructed labour (28%), and eclampsia (14%) — all conditions that require skilled clinical attendance, equipment, and drugs. All things that cost money that neither the government nor mothers currently have readily available.
The WHO estimates that Kenya's maternal mortality ratio was 530 deaths per 100,000 live births in 2020 — a figure that may worsen if financial barriers to facility delivery continue to grow.
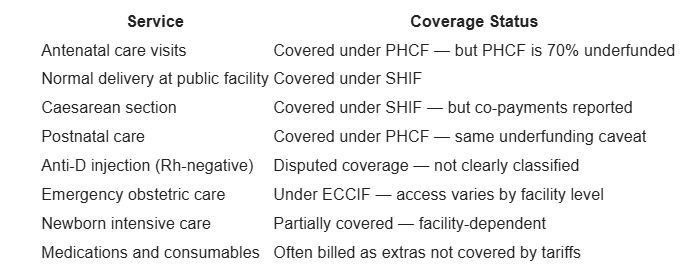
What SHA Actually Covers — And What It Doesn't
AfyaWatch254's breakdown of the current SHA maternal package:
1. The PHCF must be fully funded. A 16–30% budget allocation for the fund that covers antenatal and postnatal care is not a health policy — it is an underfunded promise. Parliament must demand full allocation.
2. SHA reimbursements must be paid on time. Facilities withholding or rationing services for fear of non-reimbursement is a direct threat to maternal health outcomes. The arrears crisis must be resolved.
3. A dedicated indigent fund must be created. Under Linda Mama, the poorest women had a clearer pathway to free delivery. Under SHA, that pathway has blurred. Women in the informal sector — who make up the majority of Kenyan women — are falling through the gaps.
4. Discharge before payment must be enforced. Hospitals detaining mothers over unpaid bills is illegal under Kenyan law. The Ministry of Health must enforce this without exception.
AfyaWatch254 Says: Free Maternity Is A Right, Not A Budget Line
Kenya's Constitution recognises the right to the highest attainable standard of health. A mother going into debt — or into a home birth — because SHA doesn't cover what it promised is not Universal Health Coverage.
It is Universal Health Insurance — and there is a difference.
We will continue tracking how SHA is failing mothers. Because no woman should die at the delivery table for lack of a functioning bureaucracy.
→ Know your rights as a maternity patient under SHA:
You have the right to be discharged after delivery without paying first. If a facility detains you, report to the SHA Consumer Portal or call the MoH hotline.